They were said to have signal intensity similar to normal cortex on all sequences, this is in fact not true in most cases 7.
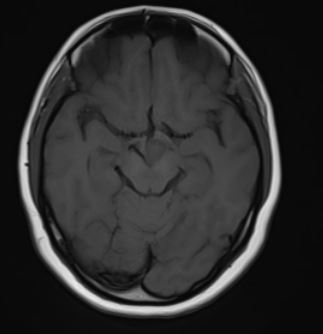
T1
hypointense to the cerebral cortex (74%) 7
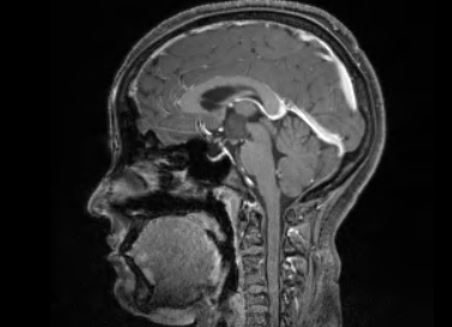
T1 C+ (Gd): no contrast enhancement
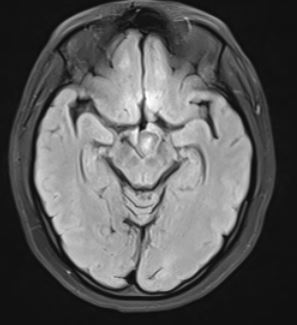
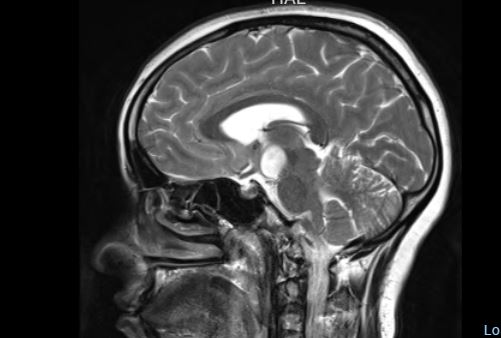
T2
hyperintense to the cerebral cortex (93%) 7
hyperintensity is more conspicuous on FLAIR
the higher the proportion of glial cells, the higher the T2 signal 3
MR spectroscopy
reduced NAA/Cr
increased myoinositol 3
increased Cho/Cr compared to the amygdala has also been reported
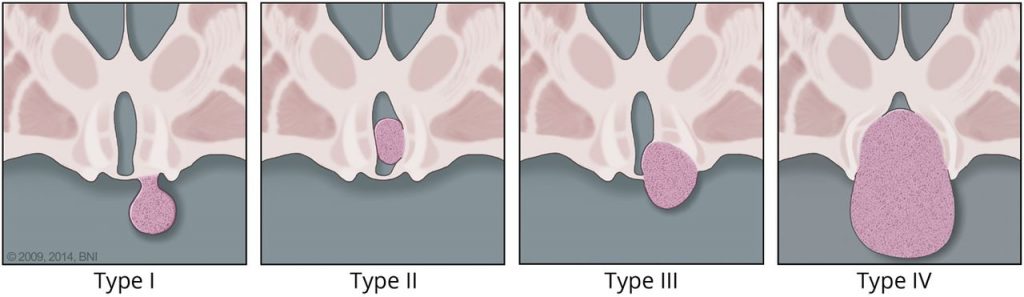
Delalande Classification of Hypothalamic Hamartomas
Type I lesions have horizontal attachment inferior to floor of the third ventricle.
Type II lesions have vertical attachment to the wall of third ventricle and are above the floor of the third ventricle.
Type III lesions have horizontal and vertical attachments above and below the floor of the third ventricle.
Type IV lesions are considered “giant” with volume 8 cm3 or larger
The differential diagnosis is broadly that of suprasellar/hypothalamic lesions, although the imaging characteristics of hypothalamic hamartomas significantly reduce the differential.
Hypothalamic-chiasmatic glioma is the main differential. Most other lesions encountered in the region either have markedly different signal intensity or demonstrate enhancement.